Why DME order intake remains highly manual
Intake teams juggle high document volume, inconsistent referral formats, and pressure to enter orders quickly. Many organizations lack a single inbox—fax servers, shared email, portal downloads, and EHR printouts each feed separate habits and spreadsheets.
Manual intake creates variability. One coordinator may catch a missing signature; another may advance an incomplete order. Without standardized queues and audit trails, managers struggle to measure deficiency rates or intake cycle time accurately.
Intake channels and disconnected workflow problems
Effective automation starts by mapping every channel that creates or receives an order record.
When channels are disconnected, duplicate patients and duplicate orders increase. Billing may receive deliveries before intake documentation is complete. Authorization teams start work on orders missing payer details or diagnosis context. Without channel-level metrics, leaders cannot tell whether fax volume, portal adoption, or EHR integration gaps drive the backlog.
- Inbound fax with prescriptions, chart notes, and cover sheets
- Email attachments from referral sources and internal staff
- Referral portal uploads and web form submissions
- EHR exports and HL7/FHIR messages where available
- Phone and voicemail follow-ups that require structured callbacks
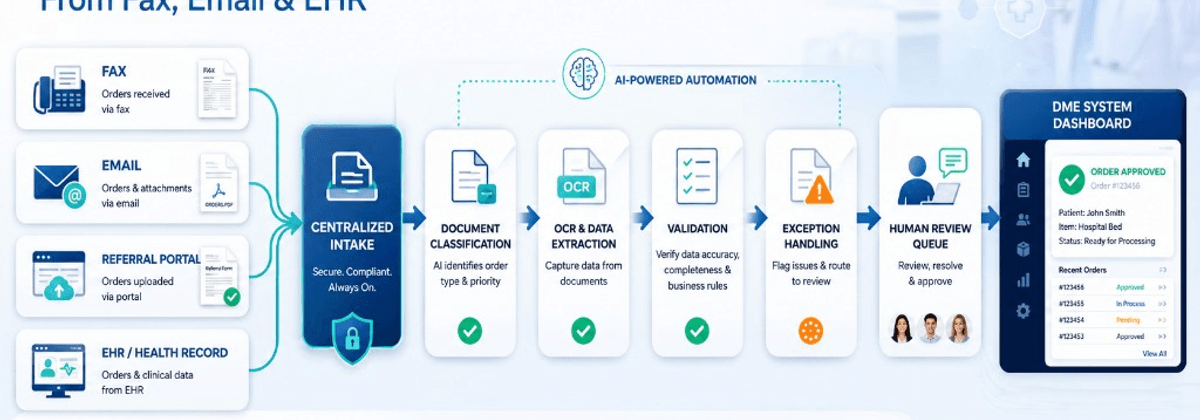
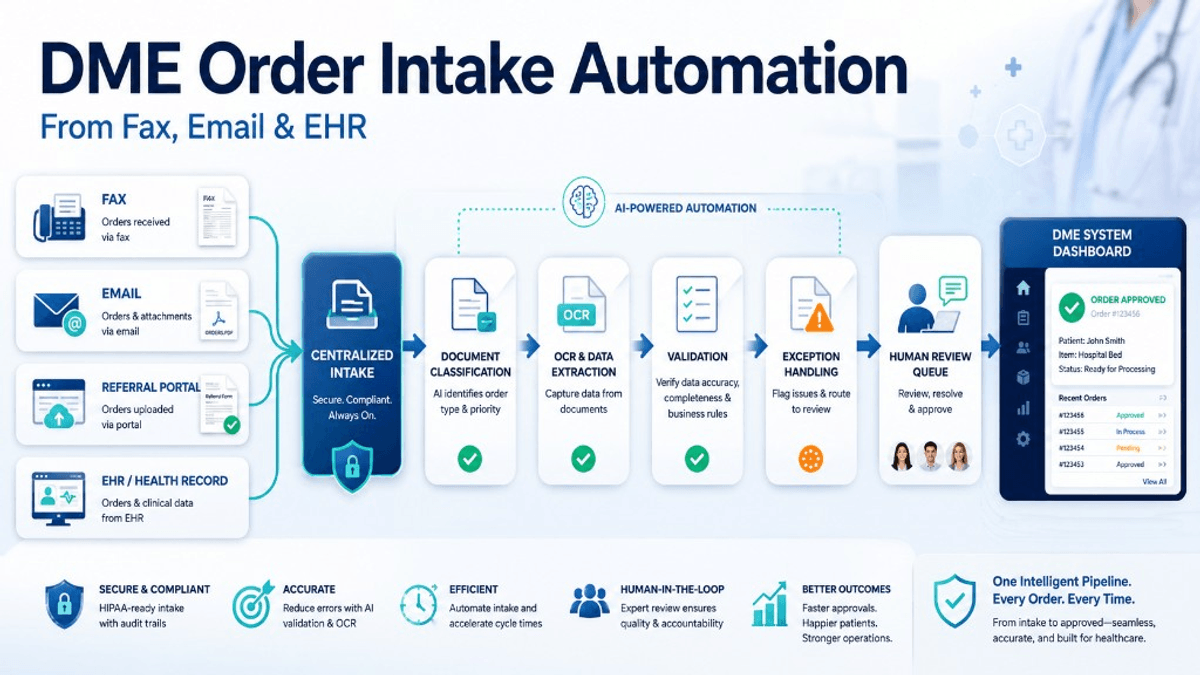
Capturing fax, email, portal, and EHR referrals
Centralize capture into a monitored ingestion pipeline. Fax images, email attachments, and portal files should land in a controlled repository with source metadata—sender, timestamp, channel, and referral source identifier.
EHR integrations may use APIs, scheduled exports, or middleware when real-time interfaces are limited. Clinic-to-DME referral patterns that reduce re-keying often combine EHR exports with fax capture and patient matching before orders enter operational systems.
KyszTech helps with healthcare integrations and AI document processing workflows that normalize multi-channel intake without replacing operational platforms.
Document classification, extraction, and validation
Classification separates prescriptions, chart notes, insurance cards, CMNs, sleep studies, and cover sheets. Accurate classification drives which extraction models, checklists, and reviewers apply next. Rules-based classifiers handle predictable layouts; machine learning assists when layouts vary widely. Low-confidence classifications should route to human reviewers rather than auto-advancing.
OCR and field extraction pull structured data from unstructured documents: patient name, DOB, address, insurance ID, referring physician, diagnosis codes, requested HCPCS or product descriptions, and order dates. Extraction quality varies by scan quality, handwriting, and template diversity. Confidence scores per field help reviewers focus on uncertain values instead of re-reading entire faxes. KyszTech supports AI document processing with human review for low-confidence fields.
Early deficiency detection saves downstream rework. Automation can compare received document types against payer and product checklists, detect missing pages in multi-page faxes, and flag absent signatures or dates. When documents are missing, workflows should generate structured requests to referral sources and pause or branch the order until responses arrive.
Validation applies operational rules: required fields present, date formats plausible, insurance ID checksum patterns where applicable, and product requests aligned with referral type at a high level. Validation supports staff review; it does not replace clinical or coding authority. Invalid or ambiguous records advance only after human confirmation.
Duplicate detection, exception queues, and system write-back
Duplicate records remain a persistent DME problem. Matching algorithms should compare demographics, insurance identifiers, open orders, and referral timestamps before creating new patient profiles or order shells. Potential duplicates should land in a merge or review queue—not silently overwrite existing records.
Exception queues are the operational heart of safe automation. Categories include low-confidence extraction, missing documents, duplicate suspects, payer not recognized, and referral source not mapped. Each queue needs owners, ageing visibility, and escalation rules so orders do not stall silently.
After human approval, validated data should write into Brightree or other operational systems through APIs, middleware, or controlled import patterns. Write operations must be logged with before-and-after values for auditability. KyszTech provides healthcare integration services for Brightree-compatible workflow connections.
Human review, HIPAA controls, and audit trails
Define thresholds that trigger mandatory review—for example, extraction confidence below an agreed level, paediatric orders, high-cost equipment categories, or payer plans with historically complex requirements. Review screens should show source documents alongside extracted fields so approvers can confirm quickly without re-opening fax software.
Log document receipt, classification, extraction, reviewer actions, and system writes. Restrict access by role and integrate ingestion pipelines with encryption and retention policies aligned to organizational HIPAA obligations.
Organizations must evaluate BAAs, subprocessors, and state requirements independently—automation vendors and integrators should support controls, not define compliance posture.
Metrics and implementation roadmap
Track intake cycle time, auto-classification accuracy samples, reviewer minutes per order, deficiency rate at intake, duplicate creation rate, and channel-specific backlog ageing.
Weeks 1–2: Map channels and baseline metrics. Weeks 3–6: Pilot fax and email ingestion with classification and human review. Weeks 7–12: Add portal and EHR feeds, duplicate detection, and Brightree write-back with monitoring.
Begin with a focused workflow assessment if intake volume spans many product lines. Contact KyszTech to discuss intake automation aligned to your referral mix and systems.