What are HME and DME operations?
HME and DME operations cover everything required to move a patient from referral to delivered equipment, ongoing resupply, and reimbursement. That includes intake, clinical and payer documentation, insurance workflows, product selection, fulfilment, patient setup, billing, and recurring patient engagement.
Unlike retail fulfillment, DME operations depend on payer rules, medical necessity documentation, HCPCS-related workflows, and proof-of-delivery requirements. A single order may touch intake coordinators, clinical reviewers, authorization specialists, warehouse teams, drivers, billing staff, and resupply teams—each working from partially overlapping data.
Operational leaders typically measure success through order cycle time, documentation completeness, authorization turnaround, delivery performance, claim acceptance, denial rates, and patient retention on resupply programs. Automation targets the repetitive steps between those outcomes—not the clinical or compliance decisions that still require trained staff.
Why order growth exposes operational bottlenecks
Many HME/DME businesses scale revenue faster than they scale process discipline. Referral sources increase, payer mix shifts, product lines expand, and resupply programs add recurring volume—all while intake still relies on fax review, spreadsheets, and inbox triage.
Growth exposes bottlenecks that were tolerable at lower volume: missing signatures discovered late in the workflow, authorization follow-ups tracked in personal notes, duplicate patients created across systems, and billing teams receiving orders that were never fully documented for claim readiness.
The result is not just slower processing. Teams experience unsafe workload pressure, managers lose visibility into ageing orders, and executives see margin erosion from rework rather than from demand itself. Before selecting software, providers benefit from mapping workflow stages and manual touches through a structured operational assessment.
- Intake backlogs when fax and email volume spikes
- Authorization delays when payer rules vary by product and plan
- Duplicate entry between fax workflows, CRM notes, and operational systems
- Billing holds caused by documentation discovered after delivery
- Resupply leakage when patient outreach is manual and inconsistent
Not sure which HME/DME workflows should be automated first? Start with a workflow assessment covering intake, documentation, authorization, fulfilment, billing, resupply, and system integration.
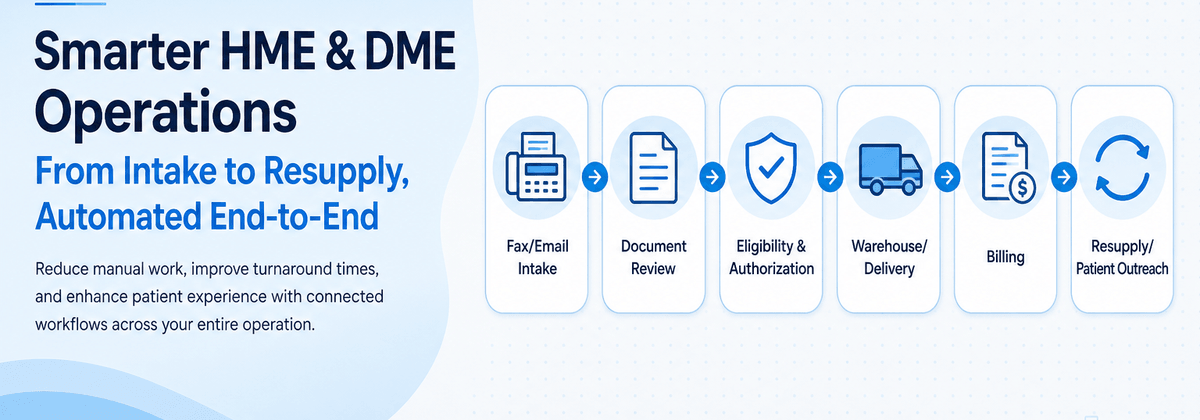
The complete HME/DME order lifecycle
A typical DME order lifecycle begins with referral capture and ends with reimbursement, resupply, and ongoing patient communication. Each stage has distinct data requirements, owners, and exception paths.
Automation is most effective when it follows the lifecycle rather than a single department. Connecting intake improvements to authorization, fulfilment, and billing reduces the compounding errors that appear when each team optimizes in isolation.
- Referral and order intake
- Prescription and supporting-document collection
- Eligibility and benefits verification
- Prior authorization and medical necessity review
- Product qualification and order validation
- Fulfilment, delivery, setup, and proof of delivery
- Billing, claims, denials, and reimbursement
- Resupply and recurring-order management
- Patient, physician, and referral-source communication
Order lifecycle: intake through resupply and communication
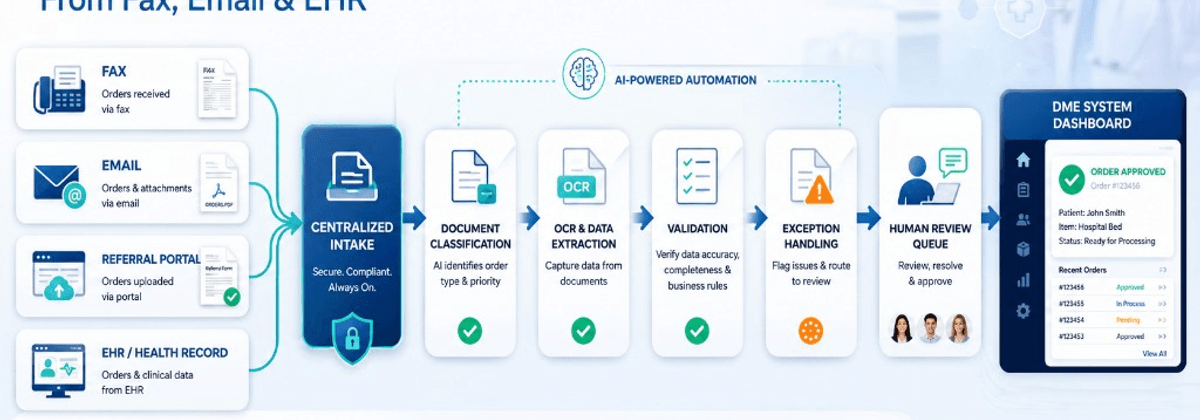
Order intake is often the first bottleneck. Referrals arrive as faxed prescriptions, emailed PDFs, portal uploads, phone messages, and EHR exports. Staff classify documents, identify patients, and enter data into operational systems—sometimes retyping information that already exists elsewhere. Automated intake focuses on capture, classification, extraction, duplicate detection, and exception queues—not on bypassing review. See our dedicated guide on DME order intake automation for channel-specific approaches covering fax, email, portals, and EHR referrals.
DME orders require more than a prescription. Payers and accreditation expectations often include chart notes, face-to-face documentation, sleep studies, CMN forms, and signatures with appropriate dates. Missing or incomplete documents are among the most common causes of downstream delay. AI document processing can classify incoming files, extract key fields, detect missing pages, and route low-confidence items to human reviewers. AI supports operational review—it does not replace clinical or compliance judgment on medical necessity or coding decisions. Automation should track document status visibly: received, under review, deficient, requested from referral source, and ready for next workflow stage.
Eligibility and benefits verification confirm active coverage, plan details, and benefit parameters before expensive fulfilment or authorization work proceeds. Workflow automation can standardize when verification runs, what data is captured, and how results attach to the order record. Organizations must evaluate payer-specific requirements and contractual obligations—automation assists operational consistency; it does not guarantee coverage or payment outcomes.
Prior authorization remains one of the highest-friction stages for many DME product lines. Requirements vary by payer, plan, HCPCS code, and clinical scenario. Automation can help determine when authorization is likely required, assemble checklist-driven packets, monitor status, send reminders, and prevent duplicate submissions. Human approval remains essential before submission and when clinical questions arise.
Before fulfilment, teams validate that the ordered product matches clinical documentation, payer rules, patient history, and inventory availability. Automation can apply rule-based checks: required fields present, diagnosis and product alignment at an operational level, duplicate open orders, and missing authorization references.
Fulfilment connects warehouse operations, routing, patient scheduling, setup instructions, and proof-of-delivery capture. Integration between operational systems, routing tools, and mobile capture workflows reduces manual status updates. Billing teams depend on documentation readiness, accurate demographics, valid authorization references, and proof-of-delivery availability. Automation can support claim readiness checks, work queue prioritization, denial classification, and corrected-claim workflows—always with human review for compliance-sensitive decisions.
Resupply programs—especially CPAP and other recurring supplies—depend on eligibility timing, patient engagement, and repeat order creation. Automated resupply workflows combine eligibility checks, patient communication across voice, SMS, email, and portal channels, confirmation capture, and order creation—with human escalation for clinical or coverage questions.
Patient and referral-source communication affects resupply conversion, document turnaround, and repeat referral volume. Automation can send status updates, document requests, and resupply reminders through approved channels while logging communication history. Voice AI and structured messaging can reduce repetitive outbound effort when human escalation paths are defined.
- Authorization requirement rules by payer and product category
- Checklist-driven supporting-document assembly and submission tracking
- Automated follow-up tasks for pending authorization requests
- Exception queues for denials, partial approvals, and peer-to-peer requests
- Proof-of-delivery capture and billing readiness coordination
Where AI and automation can help
Automation delivers the most value on repetitive, rules-heavy, document-heavy work: classifying faxes, extracting patient demographics, matching orders to existing records, monitoring authorization status, updating work queues, and preparing billing readiness checklists.
AI document processing, workflow orchestration, and integration middleware can connect steps that currently depend on email handoffs. None of this eliminates human review for low-confidence extractions, clinical questions, payer disputes, or compliance decisions.
Providers exploring scalability without proportional headcount growth should focus on straight-through processing, exception-based operations, and centralized visibility while maintaining quality controls and manageable workload design.
- Document classification and field extraction with confidence scoring
- Duplicate patient and duplicate order detection
- Exception queues instead of inbox chaos
- Authorization and documentation task orchestration
- Operational dashboards for ageing and ownership visibility
- Integration monitoring with alert paths for failed sync jobs
Brightree, eClinicalWorks, fax, EHR, payer, and CRM integrations
Most U.S. HME/DME providers already run operational platforms, EHR interfaces, fax infrastructure, payer portals, and CRM or referral-tracking tools. Replacement is rarely the fastest path to improvement. Integration and workflow automation around existing systems usually is.
Brightree is widely used for HME/DME operations. KyszTech provides Brightree-compatible workflow automation and integration services—we are not claiming any official Brightree partnership unless separately verified on our site. Common patterns include API, middleware, and file-based connections for intake, authorization, fulfilment, and billing workflows.
Clinic-to-DME flows often involve eClinicalWorks exports, faxed supporting documents, and manual reconciliation before orders exist cleanly in operational software. Integration work should focus on referral capture, patient matching, missing-document requests, and status communication without implying vendor partnerships.
Rip-and-replace projects stall when teams underestimate migration risk, retraining load, and payer recredentialing disruption. Incremental automation around current systems delivers faster operational relief with lower change risk. Middleware, event-driven workflows, and human review queues bridge gaps between fax, EHR, operational platforms, and payer channels.
Our team has experience building and supporting healthcare operational workflows that involve high order volumes, document-heavy processes, multiple external systems, insurance workflows, fax integrations, and human review queues.
KyszTech helps with healthcare integrations, healthcare AI workflows, and enterprise development for middleware, APIs, file-based exchange, and monitored fallback approaches.
Human-in-the-loop controls
Human-in-the-loop design is not a compromise—it is how DME automation remains trustworthy. Staff should review low-confidence extractions, authorization submissions, clinical documentation gaps, billing exceptions, and patient communications that fall outside approved templates.
Effective programs define confidence thresholds, role-based approvals, override logging, and escalation paths. Automation accelerates preparation; humans remain accountable for decisions that affect patient care, payer compliance, or revenue integrity.
- Confidence thresholds for extracted fields and classifications
- Role-based approval before authorization submission
- Mandatory review queues for clinical and payer-sensitive documents
- Override logging with user, timestamp, and reason capture
- Escalation paths for exceptions that automation cannot resolve
Security, HIPAA, auditability, and access control
HME/DME automation must protect patient information across ingestion, storage, processing, integrations, and audit logs. Organizations are responsible for evaluating their own HIPAA, BAAs, payer, state, and contractual obligations—software alone does not guarantee compliance.
Security-conscious design includes encryption in transit and at rest, role-based access, least-privilege integration credentials, retention policies, and immutable audit trails for document and workflow actions. NIST Cybersecurity Framework guidance and HHS HIPAA resources are useful references for control design.
- Role-based access aligned to intake, clinical, billing, and admin functions
- Audit logs for document views, extractions, approvals, and integrations
- Secure handling of fax and email ingestion pipelines
- Monitoring for failed jobs, unauthorized access attempts, and data export events
- Vendor and subprocessors governed by appropriate agreements
Operational metrics, phased roadmap, and next steps
Automation programs need operational metrics tied to workflow outcomes—not vanity counts of documents processed. Leaders should baseline metrics before implementation and review them by team and product line.
Attempting to automate every stage simultaneously overwhelms staff and obscures ROI. A phased roadmap prioritizes high-volume friction points with clear ownership and measurable baselines. Phase 1 typically focuses on intake capture, document classification, duplicate detection, and exception queues. Phase 2 connects authorization and documentation orchestration. Phase 3 extends to billing readiness, resupply engagement, and integration monitoring.
HME/DME operations automation is an operational discipline—not a single software purchase. U.S. providers that connect intake, documentation, authorization, fulfilment, billing, resupply, and communication while preserving human review can scale more predictably without forcing a platform replacement. For deeper intake guidance, see our DME order intake automation article as a companion to this lifecycle guide.
Start with a structured workflow assessment to identify quick wins versus strategic investments. Contact KyszTech to review intake, documentation, authorization, fulfilment, billing, resupply, and integration priorities aligned to your systems and team capacity.
- Intake cycle time from receipt to validated order record
- Documentation deficiency rate before fulfilment and billing
- Authorization turnaround and pending-age distribution
- Order ageing by stage and owner; manual touches per order
- First-pass billing readiness and denial rates by category
- Days 1–30: Map order sources and baseline ageing and deficiency rates
- Days 31–60: Pilot intake automation with human review and audit logging
- Days 61–90: Expand authorization orchestration and integration monitoring
- Quarter 2+: Billing readiness queues, resupply automation, and dashboard visibility
Not sure which HME/DME workflows should be automated first? Start with a workflow assessment covering intake, documentation, authorization, fulfilment, billing, resupply, and system integration.